This year will also mark 25 years since the Beijing Declaration and Platform for Action adopted at the Fourth World Conference on Women (Beijing, 1995). This conference sought to remove all the obstacles to women’s active participation in all spheres of public and private life through ensuring women a full and equal share in economic, social, cultural and political decision-making.
In the spring the creators of the cult “Sex and the City” are preparing to shoot a sequel to the series, which has already become a classic. The familiar heroine-friends will tell us a fascinating story about the life of a modern woman after 50 years. Sarah Jessica Parker, Kristin Davis, Cynthia Nixon and Kim Cattrall have changed a lot since their first appearance on small screens. But that makes it all the more interesting to see how they look now, and to find out what treatments help them maintain Kristin Davis bad plastic surgery their beauty. Carrie Bradshaw closet: making your dream come true without losing space. Surgery to reshape the nose was performed by those actresses of the show, who confirmed their participation in the announced project. Sarah Jessica Parker, Kristin Davis and Cynthia Nixon. But Kim Cattrall, who unfortunately refused to participate in the upcoming shoot, did not resort to rhinoplasty.
As the buzz around Universal Health Coverage continues to build, bringing on board the gender lens to policy deliberations cannot be more timely. In this common spirit, a number of advisers and researchers were brought together in Nairobi in February 2019 and developed this guide (Adopting a gender lens in health systems policy: A guide for policy makers) which does a few things:
Defines what a gender-equitable health system might look like
Provides a set of benchmarks that health policy makers can work towards
Features case studies from a range of countries, including Cambodia, Democratic Republic of Congo, Kenya, Liberia, Malawi, Sierra Leone, South Africa, Tanzania and Uganda. These illustrate how decision making that does not take gender into account leads to sub-optimal health systems and provide practical examples of strategies that have been effective in addressing gender barriers in health systems.
Lists further resources which are accessible online
Gender is everyone’s business
To start with, it is important to note that gender is everyone’s business and not only about women and girls and excluding others as is often misinterpreted. Owing to gender biases, norms, and power relations, some groups of people are often not factored in decision making processes and this means that their needs and rights are not identified, recognized or prioritized.
Likening the health system to that of a computer, it has both the hardware and software system. The hardware components include the six building blocks identified by the World Health Organization (WHO). These building blocks include: health service delivery, governance, medical products and technology, health systems financing, human resources and health information systems. The software system on the other hand is hard to see but it is critical as it cements and informs the success of work on the building blocks and includes relationships, values, trust, and power. As the authors in this guide: state: “Both the hardware and software of the health system are affected by gender. Gender norms, roles, and relations are also shaped by the health system.”
The building blocks
On the second page of this very enlightening guide, the authors delve deeply and even graphically into what gender-equitable health systems look like, providing detailed information on the aforementioned six building blocks. Take for example the importance of providing accessible, acceptable, affordable and available health services as a core function of a health system. Further down that page as you’ll see when you read, there is an illustration of how the divergent needs, rights, access, and experience of health services for men, women, and people of other genders affect the range of demand- (patient-led) and supply-side (health service-led) factors. For instance, a case study from Kibuku district in Uganda demonstrates how health facilities are making life more bearable for physically disabled women.
The second building block is very important as it focuses on health workers who are the backbone of the health system. The policy brief in this section outlines very fundamental recommendations for policy makers based on experience from the different implementers as reflected in the case studies and recommended resources like the WHO (2011) Gender mainstreaming for health managers: a practical approach.
An inclusive health system should, by definition, place fairness and equity at its core. However, many health systems’ governance structures and processes fall short of their potential when it comes to gender equity. There is a lack of goal setting for higher representation of women in leadership and policy spaces in the form of targets, quotas and affirmative action. The guide underscores the key issues in gender and accountability and also suggests ways in which these issues can be addressed by policy makers like ensuring gender balance and gender sensitivity of governance structures at all levels down to the facility and community level.
The brief also features a very well written and interesting case study on “Gender analysis of community health data in Kenya”. It documents the direct impacts of gender on the quality of data reported by Community Health Volunteers due to gendered barriers in data collection. Case in point, what many would regard as a “simple” issue like the fact that some health issues are perceived to be the domains of men or women; consequently, inform trends like that of Community Health Volunteers collecting data from women. This leads to men’s perspectives missing from the data routinely reported. These gendered elements of data collection impact on dimensions of data quality such as accuracy, completeness, reliability and confidentiality. There’s a wealth of resources put together by the authors of the brief on the same. Check it out!!
Finally, we turn to health financing which is the accumulation and allocation of funding by and within the health system to ensure service quality and access is very important. As quoted in the guide:
The extent that financial protection is available to different groups needs to be considered, in addition to how out-of-pocket expenditure is experienced differently by men, women, and people of other genders. This affects policy makers’ ability to deliver Universal Health Coverage.
Make policy change
Policy makers can give women their rights on international women’s day by taking up this recommendation to:
Ensure that financial protection packages (i.e. prepaid health services under Universal Health Coverage schemes) include essential and routine sexual and reproductive health services, such as childbirth and emergency obstetric care, family planning, cancer care, such as for prostate cancer, and safe abortion.
Gender mainstreaming is a challenging and ambitious process but we have no choice if we hope to achieve a gender equitable health system and this guide is a gift to all policy makers who are trusted to lead the process.
As researchers, many of us worry about the value of our work and interventions, and even about whether we are doing more harm than good. These lurching feelings of discomfort could begin to be addressed through ethical reflection, review, and analysis, but all too often we see this as something that occurs somewhere else: in elite spaces, among people higher up, behind closed doors, or in institutional review boards.
The new guide to ethics in health policy and systems research was started with this in mind; with an aim to be a resource for health systems researchers to find and share information to support practical, applied, day-to-day ethics.
There are very few guidelines and papers which deal directly with the ethics of health systems research. As mentioned on the website, existing guidelines and research ethics committee members’ training tends to focus predominantly on the ethics of biomedical research. This is challenging for health policy and systems research, which often operates at system or population as opposed to individual level. This resource aims to bring together the available evidence on ethics and health systems research and casts the net wider for papers, case studies and other outputs that can help illuminate some of the challenges we all face.
The website is divided into different sections: the Overview section provides information on issues such as ethics, power, positionality, and progress. The section on the Day-to-day process of research highlights some of the common challenges that health systems researchers face and provides references which explore these issues in greater detail.
Under, ‘Choosing questions, study designs and methods’, a major issue raised is that much funded research in low- and middle-income countries focuses on a narrow set of questions related to service delivery and scale up rather than on broader health system research questions that are responsive to local needs or focused on equity.
“Strong respectful relationships – between investigators, between researchers and the communities and institutions that they work in, with policy makers, practitioners and other users of research – are key to research success and vital to ethical practice.”
Data collection and the issues that surround it such as the complex interplay between vulnerability and agency are not new subjects to researchers. This section provides resources like case studies exploring the vulnerabilities of communities affected by HIV in Kenya and how ethical issues that arose in the course of the work were addressed.
“Analysing data throws up a number of ethical dilemmas for health systems researchers…including having to carefully consider the physical and socio-political positions of researchers which have implications for the entire research process, including analysis, and the importance of considering collaborators and research impact in analysis plans.”
Overall, there are a wealth of resources assembled in this website that could be valuable for health systems researchers grappling with a range of topical issues. What issues and whose views are heard and prioritized in research? Which priorities are set and through which processes? What are the power relations between researchers, funders, decision makers and users of health system? How is funding generated and spent in the creation of new knowledge? These are all issues that most health systems researchers are familiar with but don’t often think of as ethical issues and the additional lens that this can bring to our reflections. This website in exposing us to practical, applied ethics can begin to help us think through such issues.
Have a look and let the RinGs team know if you have resources you would like added to the site!!
There is a growing interest in women’s role in global health leadership. We know that women are the majority of people working to improve health outcomes; in communities, as health care workers, and in non-governmental and multilateral organizations. So why is it that when it comes to leadership positions we have a governance system that privileges men and what can we do to redress the balance?
This ground breaking collection will explore the leadership roles that women currently play in global health, teasing out the routes that women have taken to leadership, the challenges that they have faced, and what has facilitated their journey. It will bring to the fore the stories of women on the frontlines of this struggle from around the world, highlighting and complimenting these stories with theoretical and analytical explorations of the structures and systems that help or hinder the process. The aim of this book is to form a rallying call to arms to redress gender inequality and celebrate the many ways in which women are taking the lead in supporting the health of their communities internationally. It will be a must read for those working in global health or studying the topic.
We are seeking contributions based on empirical studies (e.g. quantitative or qualitative research, literature reviews, etc.) focusing on key issues related to women’s role and involvement in global health leadership in a variety of global health sectors, including: academia, health systems, global health governance, and civil society. The book will be published by Springer in 2020. We are particularly interested in authors from low- and middle-income countries.
Topics of interest include:
How gender intersects with other axes of inequality, for example race, ethnicity, age, sexuality, (dis)ability, migration status.
How women’s leadership is thwarted or supported from in a range of different contexts, positions, and starting points.
Barriers to women’s participation in leadership positions, including lack of value, recognition and respect at work; dual burden of professional work and childcare and household chores; leadership styles and influence on career advancement.
Any topic related to women’s career advancement and/or leadership.
Expressions of interest should by no longer than 500 words and can be written in the form of an abstract. Include name and organization affiliation if applicable. Submissions from any context and career stage are permitted. Please indicate which topic area your study falls under: academia, governance, health systems, or civil society.
Submit to Rosemary Morgan at RinGs.RPC@gmail.com no later than Friday 19 April 2019.
On the 28 February an international group of gender and health systems experts came together in Nairobi for a dialogue with their counterparts from the policy world. The meeting was an opportunity to look across domains of the health system that included community health, governance and access to services to identify how gender norms impede progress of the development of health systems which are people-centred and truly universal. The meeting was convened by the KEMRI Wellcome Trust, supported by RinGs and funded by the ALIGN Platform.
The meeting grew out of a growing body of research at KEMRI Wellcome Trust that addresses issues like governance, child health, nutrition, household decision making and financing from a gender perspective, capacity building to strengthen a gender analysis and a desire to engage with government action in this area. As part of this KEMRI Wellcome Trust have been active leaders in RinGs – an international network which has been supporting researchers in low- and middle-income countries to better study and communicate about this area of work.
An opening presentation from Valerie Percival outlined our expanding knowledge of how health systems are both shaped by and shape gender norms, mirroring broader inequity in society. She argued that health systems should provide egalitarian spaces for the engagement of all and promote gender equity. Our work in this area should explore how gender equity should be supported while guarding against negative backlash.
Valerie highlighted that traditional models assume that health systems are gender neutral and they don’t acknowledge the role of social norms in provider behaviour, access to services, medicines and commodities, governance, human resource management and other aspects that are central to health systems building blocks. As they are social systems, health systems software is also shaped by the norms of the societies that they are situated within, for example reinforcing problematic norms about women’s role in unpaid care. Governance structures are dominated by men with little effort to support women. Health systems engage in discriminatory actions towards women and fail men and boys in multiple ways. Furthermore, there is scepticism about whether these systems can change and too often women (including female health workers) are tasked with taking responsibility for changing the world without adequate support and acknowledgement.
But change is possible.
Efforts to tackle gender norms need to take account of neo-colonial histories and must be built in the countries involved. People in the countries under consideration need an opportunity to share knowledge and shape and lead the agenda.
Dr Mary Nandili, the Director of Nursing Services in the Kenyan Ministry of Health, explored how gender affects women’s leadership in the health system – including the ratio of women to men and the ways in which social norms have led women to be seen as the ‘helpers of men’.. In Kenya, women were traditionally found in positions related to nursing, nutrition and other therapy areas. Now, however, women are competing for the same roles as men. She argued that from 2000 onwards Kenya began to significantly increase the number of women in leadership positions and dramatically increased their influence. The gender gap has narrowed which has led to stronger leadership with more harmonious working relationships and more effective management.
Dr Joyce Mutinda, Chairperson of the National Gender & Equality Commission (NGEC), Kenya, provided insight into how law, policy and standard setting can be used to support progress towards gender and other forms of equity, inclusion and raising the power of the downtrodden. She called for health policy that is devoid of gender stereotypes, and care that policy does not further marginalise disadvantaged groups. While the constitution offers protections in relation to health this does not translate into health for all. Ensuring this is particularly difficult in the context of devolution where county governments may lack the ability to budget effectively for this, when minorities are excluded for example in remote and insecure areas, and disabled people do not have adequate access to services. She argued that gender is not about women, it is about everybody. People need to be sensitised about their rights so that they can claim them, and there is a need to comprehensively mainstream gender in the health sector to address inequality in access to services, improve quality, increase resource allocation and support the adoption of effective monitoring systems.
“Speak it out. Let’s learn from each other to make health systems friendly and responsive to all people including minorities.”
Dr Joyce Mutinda
‘My work is to fight’ says Dr Joyce Mutinda, Chairperson of Kenya’s National Gender and Equity Commission. What an amazing woman, challenging us to find ways to transform health systems to be gender equitable. #gendernorms#healthsystems@RinGsRPC— linda waldman (@linda_lindaw) February 28, 2019
https://www.youtube.com/watch?v=oPRyB_tDURM
Access to services for marginalised groups
https://www.youtube.com/watch?v=liy3weVnZ2k
The view from researchers
Rachael Rebecca Apolot explained how in Uganda a community scorecard project on maternal health highlighted how women with walking disabilities faced difficulties in accessing services and unaddressed psychosocial needs. Services were physically inaccessible with steps, chairs and beds that were too high and toilets in which women had to crawl on the dirty floor. Transporters were reluctant to carry women to the health centre and over-charged disabled women. Having to travel to the health centre with a carer increased the costs of transport. Women were often aggressively questioned by health workers about their sexuality. This was underpinned by the norms that disabled women should not have a sexual life or have children. Community norms led to their marginalisation – as people thought that they may curse them. Discriminatory attitudes in the health system added to the troubles of women who were dealing with discriminatory norms in other areas of their lives.
Chandani Kharel explored gender in the workings of the Health Facility and Operation Management Committees of Nepal. These committees were set up to ensure community participation in primary health care. While these committees were able to recognise marginalised groups (such as women and Dalits) their workings were still subject to social hierarchies and gendered norms that impeded their function. Women’s representation was often tokenistic which emphasizes the need to foster true inclusion.
Returning to Uganda, gender norms also impeded access to maternal health services for migrant women from communities of labourers on sugar cane plantations. Richard Mangwi explained how his research explored how social norms prevented migrant women seeking timely care, as they were told that bearing the pain of labour without making a fuss was a sign of strength. In health care settings anti-migrant sentiment and women’s inability to speak the local language were a barrier to accessing services.
Speaking from the Kenyan perspective Chi-Chi Undie argued that every client has a gender identity and this shapes the nature of access to services by opening up or constraining opportunities. Her focus was on children and young people seeking services for sexual and gender-based violence. Children are constructed as vulnerable and this can improve service access. However, it may mean that children have to be accompanied by their parents – even when they would rather see a health professional alone. She talked about how violence against children and violence against women are often linked. Mothers may have experienced violence themselves or may require psychological assistance if their children have been hurt. In addition, social norms prescribe that even within the health system, mothers are required to lead in a caring role which is a further burden upon them. This points to the importance of an integrated and sensitive approach to care related to sexual and gender-based violence.
The view from the audience
A gender lens is important in considering the needs of all people including those not generally thought to be disadvantaged such as male migrants. We need to consider gender norms because they help shine a light on the areas we have neglected. For example, it is assumed that men don’t need services, however many fail to seek care because of norms around masculinity. Sometimes people don’t seek care because of provider behaviour which is directly related to gender norms. If we don’t consider gender norms we will fail to achieve Universal Health Coverage and we will leave some sections of the population behind.
Adolescents, by virtue of their age, face barriers in access to services – highlighting the intersection gender and age. They have to go to school and services are not always friendly or designed to meet their needs. Responsive health systems need to consider gender because the way boys access health services is different to girls as a result of norms and socialization. The health system tries to create safe spaces for adolescents, but this may keep them separate from other people and add to the vulnerability and stigmatisation that they face.
The urban poor have systems of authority and accountability that are separate to the state; for example, there are gangs, informal providers etc. These systems can stop people accessing the services that they require. Often the urban poor are seen as a problem and lack appropriate legal statuses which in turn contributes to a lack of state accountability for their rights. We need to think beyond clinical services to how environmental hazards, a lack of sanitation and living in ‘legal grey areas’ affect their health needs.
Community health systems
https://www.youtube.com/watch?v=08Ik7XlxMGE
The view from researchers
Lilian Otiso led us through research that implemented quality improvement in various counties in Kenya. She noted that the tools that Community Health Volunteers are equipped with do not adequately enable them to consider issues of gender and other variables such as age.
Through their work with maternal and child services they identified instances where Community Health Volunteers helped challenge norms. For example, their teams realised that adolescent mothers had difficulties in accessing services because of poor provider attitudes, and that older women were served first ion health facilities. They subsequently created special referral cards for them and worked with health centre staff to make services more welcoming for the young mothers. The Community Health Volunteers noted that in certain cases, men were the household heads as well as the primary carers. They supported one man, for example, to take his four children to the health centre which he didn’t know he was allowed to do because primary health facilities are generally regarded as ‘women’s spaces’. The Community Health Volunteer helped him to feel comfortable with this and as a result his children were immunised and treated for undernutrition.
https://www.youtube.com/watch?v=9l9KWfjaHbw
Sally Theobald presented work by Haja Wurie and others in Sierra Leone. They found that there was a heavy investment in hiring Community Health Workers post-Ebola to rebuild trust between the community and the health system. Nonetheless, gender norms affected who was trained as a Community Health Worker. Although the government deliberately tried to recruit women because they wanted workers who could respond to maternal health needs, more men got employed as they were more likely to have the appropriate level of education. Also, women faced challenges in blending community, paid and domestic work and some husbands didn’t allow their wives to do the job. Community Health Workers are strategically placed to alter gender norms but are also subject to them themselves as they are part of the community within which they are working.
In Uganda David Musoke’s work uncovered that although the role of community health workers was supposed to be gender neutral, in fact, they conformed to gender norms in the ways that they delivered their tasks. Men did the emergency work, transportation and physical work such as ditch digging. They had access to motorbikes whereas the female CHWs did not. Women were more involved in the maternal health work and were more available in the community as they spent more time in the home when men were out working. David also discussed the need to take into account the gender of Community health Worker in the design of community health programmes, as people often want to see a provider of the same sex.
Presentations by both Sally (on behalf of Haja) and David additionally highlighted the utility of innovative research methods and approaches such as use of the Photovoice technique which ‘tell the story’ from the perspective of community members. Such participatory approaches that are fundamentally about co-production of knowledge.
Ms Charity Tauta, Deputy Head of the Community Health and Development Unit in the Ministry of Health, Kenya, argued that meetings like this are very important for policy makers who are considering how to get to Universal Health Coverage. She explained that the community health policy will be reviewed later in the year and that evidence on gender will be welcomed in finalising it. She felt there was an assumption that women were better carers as they appear to be more caring, more available and more spiritual. However, this needs to be unpacked. She quoted Professor Miriam Were of the University of Nairobi, who says, “If it’s not happening at the community, it’s not happening.” Action at community level is vitally important to the rest of the health system.
To improve gender responsiveness and allow Community Health Workers to reach those who are marginalised it would be good if they could go to venues other than households such as schools and workplaces. Talking in the household can be difficult sometimes, particularly for adolescents. In Sierra Leone they do go to the market place and in Kenya they go to schools and day care centres in urban slums.
There is a need in Kenya to increase the numbers of volunteers for adequate coverage. Community Health Volunteers in Kenya are selected by their fellow community members based on trust and perceived ability to manage health issues. However, since devolution it is unclear how much support and capacity development are being provided to them and this should be evaluated. The issue of volunteerism and free labour which is expected from Community Health Workers/Volunteers was also raised by the audience and the need to consider including them in the government payroll.
It was thought that supportive, problem-solving supervision would help Community Health Workers/Volunteers to overcome their own negative attitudes, for example towards adolescents and better deal with gender norms.
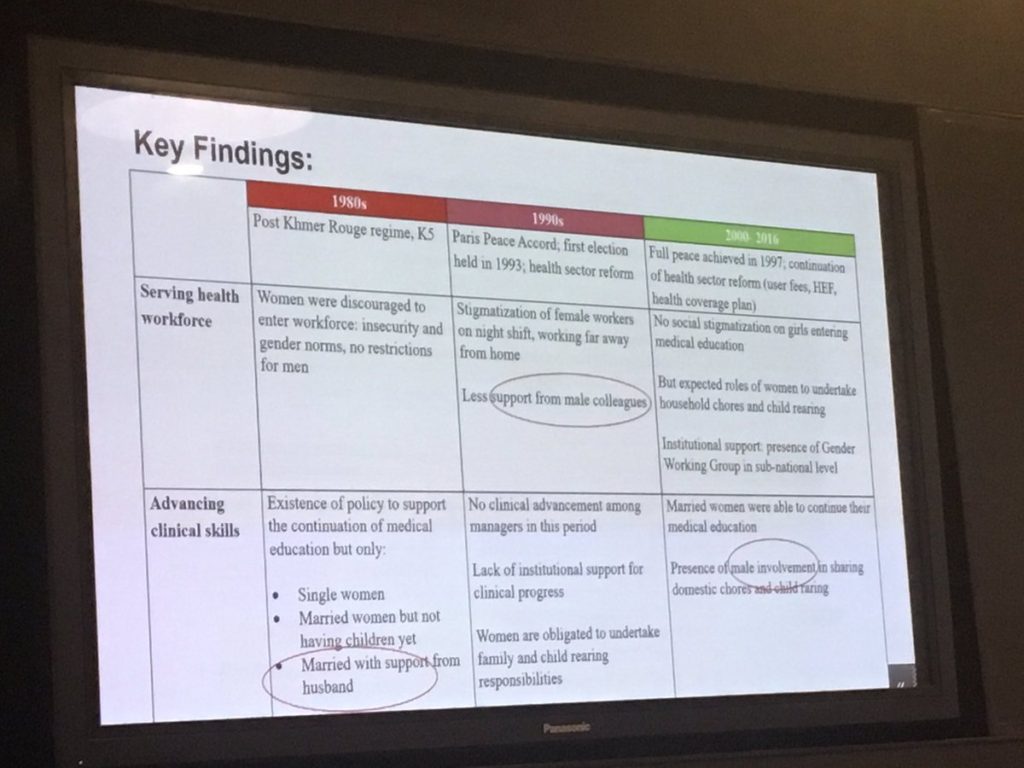
Sreytouch Vong led us through the results of her life histories work with women in the post-conflict Cambodian health system. She charted those factors that were supportive or undermining of their progression during that time. She found that if you want to support gender equality and progression for women into leadership positions, then male support is vital. This starts in the home with support to household chores and care giving for the young and the old. Female managers who have been supported by male supervisors early in their careers had made progress. However, in Cambodia many male managers still see gender as a woman’s issue and as a result they do not attend meetings that would build their skills in this area which is a weakness in the health workforce and policy planning process.
Tumaini Nyamhanga spoke about gender mainstreaming in PMTCT policies in Tanzania. Mainstreaming involves making gender central and recognising gender-based constraints such as unequal ownership of resources, harmful gender norms, imbalances in power and finding measures to correct these. However, gender mainstreaming was inadequately applied in PMTCT policy documents and organisational practices at service delivery level where most were aware of gender imbalances but did not suggest any corrective measures to transform this. He suggested that leaders in the policy realm require training to make them more gender-responsive and contribute to formulation of gender-transformative policies.
Chinyere Mbachu from Nigeria reported on her study of gender and health leadership where she found that both male and female health care managers had preconceived notions of men and women and this affected how they perceived leaders. Men believed that women don’t make good leaders because they are ‘emotionally unstable’ and lacking in focus. They also saw women as ‘followers’ and didn’t expect much from them. Even some female senior health care leaders shared these views. As a result, woman managers did not feel accepted or supported. The unequal distribution of power to men and these structures were therefore reproduced making it harder for women to occupy leadership positions in the future. Chinyere explained that when she initially started her study, her target respondents were senior healthcare managers. However, she could not identify a single woman in the senior health leadership because they simply weren’t there. As a result, she ended up conducting her study with mid-level healthcare managers so as to have both male and female respondents (as opposed to all-male respondents). This dearth of women in high-level health leadership positions in itself highlights the gendered nature of the health system, specifically the health workforce, where women generally occupy the ‘lower levels’ with their numbers sharply decreasing in the higher categories including the decision-making space.
Dr Hannah Kagiri, Head of the Gender Unit in the Kenyan Ministry of Health, explained that gender mainstreaming in the Kenyan health sector is very young and still being institutionalised. While gender is acknowledged in policies there is a lack of understanding about how to translate this into practice; and knowledge of gender norms among policy makers is low. Gender equality is often equated with reproductive health and there is not much of a focus on the non-biological social determinants of health. This leads to gender-blind policies, non-responsive budgeting and governance decisions that are insensitive to gender. There is, therefore, a need for a clear understanding of gender concepts in the Ministry and at county level. The Kenya Health and Gender and Equality policy outlines what needs to be done including better disaggregated data for decision making. For instance, while tools to collect heath data are sex-disaggregated at the point of collection, this is often removed when data are inputted into the DHIS online system. In turn, this makes the creation of gender sensitive health indicators challenging. Furthermore, there is a need to lobby for a greater budget for the Unit.
There is a need for researchers to build their skills in interacting with policy makers, for example in appropriately packaging research evidence to suit the needs of policy makers. However, the question was raised as to whether researchers are best-placed to perform this function, or whether we should engage ‘knowledge brokers’ to bridge the gap between researchers and policy makers. We also need to think about how to tell a ‘gender story’ to policy makers and others so that they can internalize the message, act on it and carry it forwards.
Policy is very bound up with politics, and development and implementation of gender-sensitive policies is often dependent on the good will of staff within the Ministry and government to make change happen. This speaks to the importance of fostering gender champions. Nonetheless many men have not been influenced by our ideas. Men need to take up this cause and support their female counterparts and help to think of effective strategies to promote gender equity. We also need to explain better how men are failed by harmful gender norms including negative masculinity and that their health suffers as a result.
Policy implications
“The policy implications of this work are complex and require concerted efforts. Recognizing this, the meeting was intended to be the start of a conversation about the way forward and building bridges rather than a solution to all the problems facing the health system. We shared across our different realms and agreed on some potential tools and interventions at different levels to achieve our vision. Evidence is crucial to the whole endeavour. We need to go beyond lip service and tokenistic approaches to change.”
Sally Theobald
Access to services: Much of the research presented clearly outlined how gender norms (and other forms of inequity) lead to exclusion from services which differs between contexts. Gender norms also shape how health care workers work and engage with patients and whether they can challenge values. We need to look at this from both a community and clinical services perspective.
Governance: In Kenya devolution has implications for the flow of money, power and resources and how these are used and negotiated for different people’s benefit. While the Gender Unit is supporting this work, we need to develop shared language and understandings throughout the health system.
Financing: Budgets need to be gender responsive. We should pay attention to gendered voluntarism at community level and which roles are paid and which are not paid. In terms of insurance we should consider who has access to it and what that means for access to health services at the county level.
Human resources: We heard about gender stereotypes around leadership and the interplay between gender, age, marriage, and professional cadre. To counteract this mentorship, supportive supervision and deconstructing a glass ceiling were suggested.
Health information systems: Gender sensitive health indicators and summary tools for disaggregation of data at local level and higher up the system are needed. But we also need the political will to use this data for change. Some of the qualitative methods used in the research presented such as in-depth interviews, life histories and photovoice can help augment this quantitative information.
Medical products and technologies: The norm for testing is often a male model, protective clothing used by health workers are designed for a male body and stock outs of essential medicines have differential impacts on men, women, boys and girls.
“Representing ALIGN, which funded the convening, I congratulate KEMRI Wellcome Trust, RinGs and the meeting participants for so thoughtfully advancing learning about a topic that has, to date, been insufficiently addressed in global health. Only by understanding the gendered nature of health systems can researchers, practitioners and policymakers overcome harmful gender norms, thereby achieving better health outcomes and improving opportunities for gender equity.”
Suzanne Petroni
Acknowledgements
This convening was funded by Advancing Learning and Innovation on Gender Norms (ALIGN), an initiative led by the Overseas Development Institute (ODI). For further information, visit www.alignplatform.org and follow @ALIGN_Project.
This meeting report was written by Kate Hawkins and also draws on notes from Linda Waldman. Some of the photos in the brief were taken by Suzanne Petroni.
How do ‘people-centred health systems’ incorporate marginalised groups?
Older models of health systems research tended to focus on the core elements, also known as ‘building blocks’ or ‘hardware’, for understanding and shaping the system – financing, health workforce, governance, medicines and other supplies, services and information systems. More recent work has explored the software of health systems, which have been described as the ‘institutions (norms, traditions, values, roles and procedures) embedded within the system’. The relationship between the hardware (the provision of clinics and medicines etc) and the software (the desire to address marginalisation or create programmes for specific health issues) are mediated by power relations. Social accountability offers a mechanism for health system users to reveal, review and redirect these power relations to achieve more equitable health outcomes.
Tools used to encourage social accountability include: citizen report cards, participatory monitoring, social audits, public hearings, and community scorecards. For any of these tools to be effective, there is a need for citizens to engage and demand accountability. Yet not all citizens are in the same position or equally able to do this: power relations also limit voice and decision-making space.
Women with disabilities
Emerging research from RinGs shows that women with disability may be marginalised from local accountability mechanisms. In Kenya women with disabilities were not asked to be part of public participation forums because people thought they couldn’t access the venue and/or considered them uneducated. As one visually-impaired woman explained,
“There are public meetings of certain kinds that we are excluded from. That’s why you find that if we go to hospitals we don’t know even where to start…we have never been invited and told this and that or gathered together with others and told these are the developments, so you find some of us are discriminated against.”
In Kibuku district Uganda, research examined the community scorecard processes and the opportunities for women with walking disabilities to be included. It found that there are no provisions within health facilities to cater for women with walking disabilities – there are no ramps so women have to crawl up the steps, there is no suitable seating so women are sitting on the floor. Here is how one woman described using the toilet,
“Our health facility does not have separate places of convenience for the disabled people. I used to go to those available but I would often find them dirty … but I had nothing to do. I would still crawl in that messed up place like that.”
These women are also excluded from accountability processes because of the difficulties they experience in securing transport. As shown in the comments above, this reinforces their exclusion, discrimination and humiliation within the health system and limits their ability to make the health system more accountable to their needs. This cannot be allowed to continue.
Moving beyond the one-size-fits-all approach
Accountability mechanisms often focus on homogenous categories of users, which can result in certain categories being elevated to the norm (i.e. male, urban, educated, heterosexual users). When an attempt is made to include ‘marginalized’ groups, token individuals – such as poor women, disabled men or adolescents – are often included to represent an entire group of ‘marginalised’ people. At the same time, little effort is made to ensure that their participation is meaningful. For example, young women may not feel able to speak up if certain men (e.g. male family members or male partners, or men who occupy a supervisory position) are in the room, or a disabled woman’s unique experience of discrimination may be disregarded for the sake of consensus. The inability of some citizens to effectively participate, or the lack of inclusion of certain citizens, means that needs and experiences specific to them are unlikely to be addressed in improvements resulting from social accountability processes.
Accountability offers communities the opportunity to influence health systems, making them more responsive to local needs. Yet, as the examples above demonstrate, there is a very real need for health systems researchers to take a critical look at social accountability mechanisms, to examine if and how marginalised people are included in such processes. This might include forming more nuanced, precise and contextually appropriate definitions of marginalisation (potentially in communities that already have poor and marginalised populations). We need more reflection on those accountability mechanisms that have been shown to work in relation to inclusion of marginalised peoples; on accountability mechanisms that move beyond tokenism and address power relations within communities and between communities and health systems. We need to be better aware of potential barriers to inclusion and how to overcome them.
There is a lot of talk about ‘people-centred health systems’ but if our accountability mechanisms only cater to certain types of already-privileged people, it seems unlikely that they will take us further towards social justice.
By Kate Hawkins, Linda Waldman, Rosemary Morgan, Sabrina Rasheed, Rebecca Racheal Apolot, Chandani Kharel, Sushil Baral, Kunle Alonge
This year we are involved in a range of panels, skills building sessions and poster presentations which bring a gender and ethics lens to health systems research. Browse the full list below and do consider coming along to meet us!
Monday 8 October
SATELLITE! Deconstructing the Gender Bias in the Health Workforce: Why Few Women Attain Leadership Positions, 12.00-14.00, ACC Room 11C
SKILLS BUILDING! Navigating day to day ethics dilemmas in health policy and systems research, 13.00-17.00, Exhibition Centre Room 24
Tuesday 9 October
SKILLS BUILDING! Using participatory visual methods to understand and support health systems with a focus on marginalized populations, 08.00-12.00, Exhibition Centre Room 19
SKILLS BUILDING! Applying intersectionality within health systems research: looking inwards and outward, 13.00-17.00, Exhibition Centre Room 22
Wednesday 10 October
PANEL! Context, gender and sustainability in introducing and scaling up essential health care packages in fragile and conflict-affected countries, 16.00-17.30, ACC Hall 2E
Thursday 11 October
THEMATIC WORKING GROUP! Incorporating a social justice lens into HPSR ethics: Implications for policy and practice in the Global South, 16.00-17.30, ACC Room 12
FILM! Are women in the Indian Sundarbans Living in the dark?, Future Health Systems stand, Exhibition Hall
Friday 12 October
PANEL! Addressing Social Inequalities Through Social Protection, 09.00-10.30, ACC Room 3B
PANEL! Amplifying marginalized voices: towards a meaningful inclusion in social accountability mechanism for health, 11.00-12.30, ACC Hall 2L
We were delighted to be part of a rich set of discussions on vulnerability, agency and resilience in a meeting organised by REACH in Oxford in May.
Sassy Molyneux and Sally Theobald
13 June 2018
Maureen Kelley kicked off the day highlighting an important paradox in health research: on the one hand research can be powerful tool for social justice in ensuring that interventions are evidence based; but on the other, there is need to protect ‘the vulnerable’ and ensure research does not worsen vulnerabilities. Current ethics guidelines do not adequately unpack or address this paradox leading to potential for all children, all women or the very poor/marginalized to be labelled as “vulnerable” and excluded from research. Yet it is these groups for whom evidence-based health interventions are most needed, raising important challenges for social justice in health. Unpacking complex intersections between dignity, vulnerability, agency and abilities in different health research contexts, and researchers’ responsibilities in designing and conducting global health research, is a key aim of the REACH collaboration. Here we share some of our key learning from the meeting:
1. CONTEXT MATTERS in how the vulnerability paradox is experienced, and contexts are fluid and changing. This can affect the vulnerabilities experienced by research participants and communities, and researchers’ responsibilities. For example, the Kenya team showed how health worker strikes in Kenya (one lasting seven months!) brought new dilemmas for researchers in face of diminished health care, with poor and marginalized groups particularly adversely affected. In other REACH study sites, where borders are contested and fluid, many research participants are migrants with specific economic and political vulnerabilities. For example, Thai colleagues highlighted that in the border regions of Mae Sot (next to post-conflict Myanmar) people are constantly shifting across borders in efforts to seek care and livelihoods. In so doing they encounter new legal and political threats. Research studies on malaria and other endemic diseases in the region offer promise of better interventions for these populations but teams face challenging dilemmas in deciding how best to respond to complex social, political and health needs.
2. COMPLEX POWER RELATIONSHIPS OPERATE AT ALL LEVELS, and are shaped by context. To support ethics practice in research and identify interventions that support social justice, complex power relations need to be unpacked and understood. For example, within households, intersecting inequities related to gender, age and education interplay to shape vulnerabilities, and are in many contexts shaped by patriarchal norms and values. These intersecting influences affect interaction with and uptake of health services, social support and research. In South Africa for example, Busisiwe Nkosi cautioned that the current emphasis by funders on girl centered interventions (for example of adolescent girls and HIV) can leave adolescent boys feeling excluded, with negative implications for everybody. As researchers learning about such influences and effects, we have to think about our responsibilities to respond: if, when, how and through whom? Complex power-relations also operate at many other interfaces in ways that have important implications for ethics practice, including between researchers of different seniority in institutions, between institutions, and between researchers and funders.
3. TRUST, VALUES AND RELATIONSHIPS are critical in negotiating how gendered power relationships play out in different contexts. Navigating these relationships is a challenging and often under-recognised job. It is often left to ‘fieldworkers’ or front line research staff from local communities to juggle the role of insider roles (as community members) and outsider roles (linked to the institutions that employ them). This critical interface role in conducting health research needs to be recognized, and staff consulted and supported in identifying and handling the multiple ethical dilemmas that can emerge.
As researchers we ourselves are part of these complex power relationships. As Bobbie Farsides noted in the discussion around the inclusion of children in research, in planning and conducting our research we should ensure that vulnerability does not function as a stop sign, but rather as an alert. This alert should be to ensure we understand the issues at stake, minimize any potential to exacerbate vulnerabilities, and work ourselves – or through appropriately placed collaborators – towards a more just society through action or advocacy. Intersectionality analysis, with its focus on power and how this plays out in multiple ways, as well as the structural factors that underpin power (political, economic, institutional) can offer a helpful way forward.
In 2016 we held our first webinar on gender, asking the question, “What part should gender play in reconstructing post-conflict health systems?” Two-years on and much has changed. There is a growing interest in applying gender frameworks and analysis in health systems research. The #metoo movement and other popular feminist actions have driven greater attention to gender equity. New conflicts and health crises have arisen in various settings prompting humanitarian emergency responses.
Our upcoming webinar does not seek to make the argument that we should focus on gender in post-conflict health systems. We feel that argument has been settled. Rather we will describe how the process of focusing on gender has unfolded in different settings and share a range of tools that interested researchers, policy makers and practitioners could use and adapt to stimulate progress towards gender equity.
We also want to hear from you. What challenges are you facing in taking forward this agenda? How can our global community of health systems researchers help in constructing the kind of evidence base that would guide good decision makers and facilitate best practice? Help us to shape the presentations by completing this short survey https://www.surveymonkey.com/r/3BHVHC5. It takes about three minutes.
Tune in for an engaging and interactive webinar with lots of audience participation.
Panellists
Introduction and survey results – Egbert Sondorp, the Thematic Working Group on Health Systems in Fragile and Conflict-Affected States
An overview of useful tools and approaches – Val Percival and Amber Warnat, Carleton University
Country case studies – Justine Namakula (School of Public Health, Makerere University, Uganda), Haja Wurie (College of Medicine and Applied Health Sciences, Sierra Leone)
The global health world does not do a good job of celebrating woman leaders. In their excellent Lancet article Rosemary Morgan and colleagues explained that of seven public health and medicine awards from diverse countries, the chances of a woman receiving a prize was nine out of 100 since their inception.
Sally Theobald and Kate Hawkins
22 May 2018
Bearing this in mind, Research in Gender and Ethics: Building Stronger Health Systems (RinGs) was proud co-sponsor of the Heroines of Health Awards, held in Geneva during the week of the 71st World Health Assembly on 20th May. Among the many people attending the event was Dr Tedros Adhanom Ghebreyesus, Director-General of the WHO.
In their introduction to the event Women in Global Health and GE Health Care wrote that:
“Women are the future. Today, women make up 75% of the global healthcare workforce and contribute nearly $3 trillion to the industry. But too often their contributions go unpaid and unrecognized – and their stories of impact go untold.”
Yemen has endured over 1000 days of war at high cost to civilians and health workers. Professor Najla Al-Sonboliis a leading researcher and Head of Paediatrics at Al-Sabeen Hospital in Sana’a was one of the honourees. Al-Sabeen remains the only centre in Yemen with a functioning Paediatric Intensive Care Unit, at a time when war has brought extreme poverty and hardship to the population of Sana’a, with children particularly vulnerable to new outbreaks of cholera and diphtheria as well as injuries. With her colleagues, Professor Al-Sonboli has worked tirelessly to provide essential care to babies and children at an incredibly difficult time. She said,
“For me, I had the chance to fly out of Yemen as many did but I preferred to stay and help my people. I thought, “if I run away and I am the head of the department, then who will stay? No one will come to work.” So, I decided to go to my hospital under fire and to try to encourage my colleagues to come, too”.
Also honoured was Anne Kinuthia who is the IntraHealth International country representative for South Sudan. She has supported the Ministry of Health and the South Sudan AIDS Commission to develop the necessary guidelines and strategic plan to inform HIV programming in the country. In the interactive panel of honourees, she shared her previous experiences of working in maternal health in the Democratic Republic of Congo, helping women to give birth, amidst rebel fire.
The Dean and the head of research from BRAC James P. Grant School of Public Health in Bangladesh, Professors Sabina Rashid and Malabika Sarker, were honoured for their work or promoting sexual reproductive health and rights within a context of fragility and unpredictability. In 2008, Sabina established a Centre for Gender and Sexual and Reproductive Health and Rights with seed funding from an UN organisation, pushing for evidence-based research, laws to stop child marriage, providing a safe space for LGBTQI communities and working to develop online resources on sensitive topics.
Sadly, war and fragility are not going away, and it is projected that the share of global poor living in fragile and conflict-affected situations will reach 46% by 2030. We need to recognise, honour, support and learn from Najla, Ann, Sabina and Malabika and all the others that work alongside them, in continuing their efforts to bring hope, health and well-being in challenging contexts. These awards reflect the respect and support from the global health community for all that they do.
Evelyn Kabia is a recipient of a RinG’s small research grant. She works at the KEMRI Wellcome Trust Research Programme (KWTRP), in Nairobi, Kenya and is a member of the RESYST consortium. Evelyn is working on a project which aims to examine the equity and pro-poorness of Universal Health Coverage reforms in Kenya. In this blog, she discusses how she became interested in incorporating a gender lens in her research work.
By Evelyn Kabia
I have a background in Nursing and I have worked in a public hospital and with non-governmental organizations where I implemented programs focusing on the alleviation of the HIV burden. I offered comprehensive HIV services mainly to female sex workers at sex worker clinics and conducted research on prevention of mother to child transmission of HIV in an urban slum settlement. My work experience made me appreciate the challenges that women face to access quality healthcare that promotes dignity and that is non-discriminatory.
My research work at KWTRP focuses on the perceptions and experiences of the people living in poverty with health financing policies that target them. These include free maternity services, user fee removal in public primary health care facilities, and the Health Insurance Subsidy Program (HISP) for the poor. Preliminary findings showed that one of the factors that limited access to skilled maternity services was perceptions of low quality of care evidenced by reports of health care worker harassment and insensitivity to the needs of pregnant women. It was also evident that people with disabilities living in poverty faced unique challenges due to limited mobility when accessing care compared to people living in poverty who were abled-bodied. These insights prompted me to incorporate an intersectional approach into the study to get an in-depth understanding of how being a woman and living with disability intersects with poverty to influence experiences with pro-poor health financing policies in Kenya.
Most of the women with disabilities living in poverty that we interviewed were single, separated or divorced. This is consistent with evidence that interactions of gender and disability result in women with disabilities having a higher likelihood of not getting married, getting married later and getting divorced earlier compared to men and women without disabilities. Women with disabilities living in poverty were therefore responsible for financially supporting their households and they were also the sole caregivers to their children. The absence of someone to assist them to watch over their children, compounded by the opportunity cost of seeking care which was lost income, that would negatively impact on their households acted as barriers to accessing care for themselves and their dependents. They therefore, forewent care to continue earning a livelihood.
Women with disabilities also face multiple layers of discrimination because of interactions between gender and disability and this leads to poorer access to health care compared to women without disabilities. In our study, this was evidenced by disabled women reporting that felt that healthcare workers had negative attitudes towards them because of their disability and the additional assistance that they required because of their disability. Some healthcare workers also questioned their right to be sexually active and their right to have children. This prejudice against disabled women resulted in a bad patient experience that discouraged them from seeking healthcare services. Women with disabilities also felt disempowered to speak out or raise complaints about the poor quality of care they received because they felt that health workers would not take their complaints seriously.
Interactions between poverty and disability and broader contextual factors also limit opportunities for people with disabilities to participate fully, economically and socially, within society. Our research reveals that negative stereotypes against women with disabilities led to their exclusion from public participation forums. Some women with disabilities were also not informed of such forums because people felt they would need assistance to access the meeting venues. This exclusion limited their awareness about health services and their opportunity to contribute to public participation forums related to health service provision.
Women and people living in poverty are disproportionately affected by disability and when gender (being a woman), disability and poverty interact, they result in multiple layers of discrimination. In Kenya, gender and disability add additional layers of vulnerability that need to be taken into account in designing pro-poor health financing interventions. Our research highlights the importance of a holistic systems approach to improving access to healthcare services.
In an effort to achieve equitable health care for all, health systems need to address the unique barriers that women with disabilities living in poverty face when accessing healthcare. Potential interventions include: expanding social assistance mechanisms to increase the amount of disposable income for the poor; building cultural competence in health service delivery, especially reproductive health services to women with disabilities; ensuring that women with disabilities living in poverty are empowered to engage in public participation; and sensitizing communities on the needs of women with disabilities living in poverty in order to reduce stigma and discrimination and to strengthen family and community support structures.
Incorporating an intersectional and gender lens to our study was instrumental in enhancing our understanding of the varying degrees of vulnerabilities among people living in poverty. Without applying this approach, the unique challenges that women with disabilities living in poverty face while benefiting from pro-poor health financing policies – due to the interaction of their social locations (gender, disability, and poverty) with underlying socio-economic and political structures – would have been overlooked. Our work, therefore, further emphasizes the importance of incorporating intersectionality and gender lens in health systems research in order to develop socially just health policies.